Click HERE to engage with AFIS on Linkedin
Over a relatively short period of time, a series of fiscal policy changes has combined to place significant financial pressure on independent schools and the families who rely on them.
The effects are not abstract. They are immediate, cumulative, and deeply personal, forcing families into difficult decisions about their children’s education, sometimes at short notice and without suitable alternatives.
For children, these are not simply financial or administrative changes. They mean disruption to education, loss of stability, and uncertainty at critical stages of development.
To understand the impact more clearly, it is worth considering how we might respond if the same approach were applied in healthcare.
A parallel system that works, until it is destabilised
Consider this:
A network of charitable independent children’s hospitals, operating alongside the NHS.
They serve a mixed group of patients:
- Some families can readily afford the fees, while others make significant sacrifices because they believe it is the right choice for their child
- Some patients are funded by the NHS, either to relieve pressure on public provision or because NHS services are not always able to meet specific needs or provide the required continuity of care
- Many exist because they provide environments, expertise and continuity of care that are not always available within the state healthcare system
In all cases, considered choices are made about what is best for each child and parental choice is respected.
No one objects to this.
Because it works.
It relieves pressure on overstretched public provision. It provides specialist environments better suited to some children. It offers stability and high-quality care for some of the most vulnerable.
And it is widely accepted because it reflects a simple principle: that parents are best placed to make decisions about what is right for their child, and that choice is respected.
A compressed sequence of fiscal policy shocks
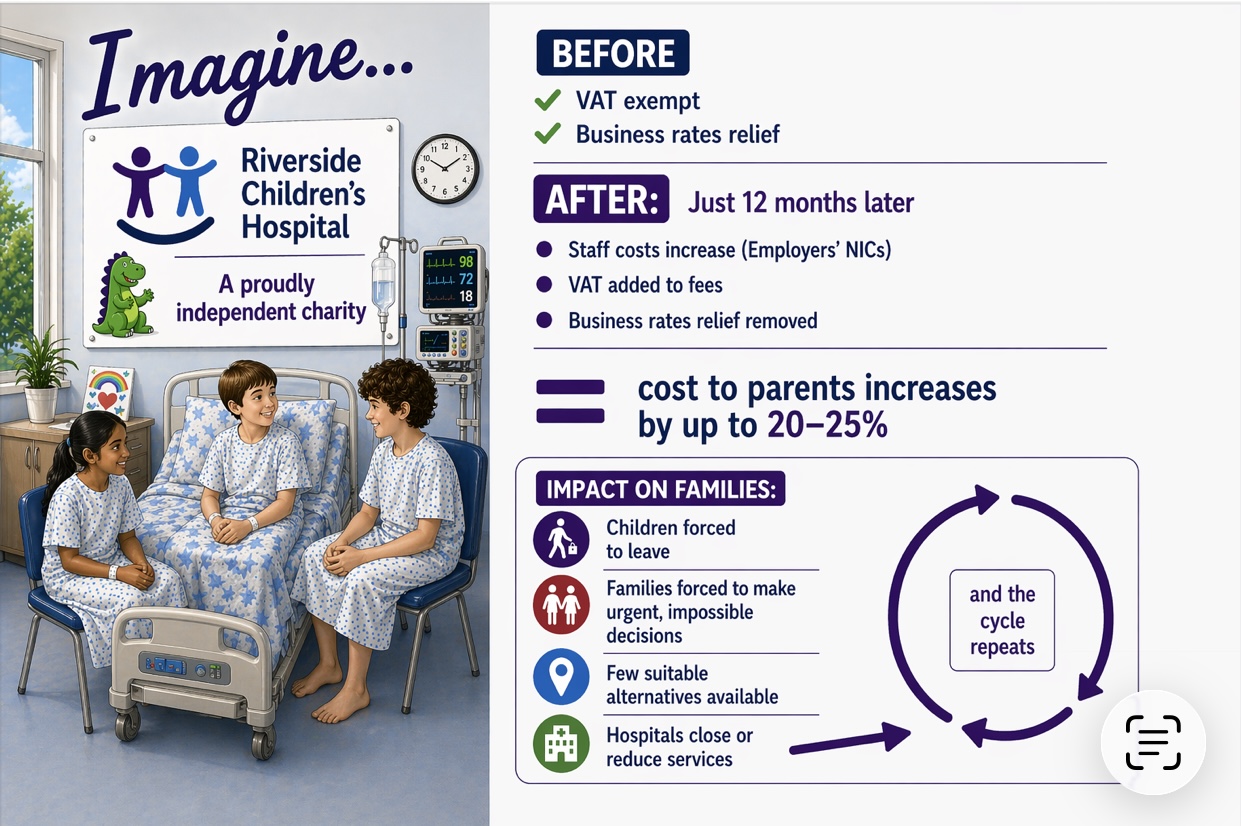
Now imagine a sequence of policy changes.
Over just 12 months, multiple cost pressures are introduced in rapid succession.
First, a major increase in staff costs. Public health providers are supported through public funding to help meet these costs. Independent providers are not.
(In education, this mirrors the increase in employer contributions to the Teachers’ Pension Scheme—from 23.68% to 28.68% in April 2024—an increase of around 20% for those schools participating in the scheme, alongside further rises in employer National Insurance contributions affecting all schools, with state schools supported through public funding while independent schools must absorb or pass these costs on to families.)
Then, a 20% tax is applied to the fees paid by families to these hospitals.
Shortly afterwards, a long-standing form of cost relief is removed specifically from this group of providers, while remaining in place for all other charities, adding further cost pressures. (No other category of charity gets singled out in this way. This is not a broad reform of charitable status, but a targeted removal applied to one sector alone).
To put this into an education context, a mid-sized independent school with a rateable value of £1 million would previously have benefited from around 80% charitable relief.
With the standard multiplier applied, the removal of that relief could add around £400,000 per year to its cost base.
Larger schools, or those in higher-value areas, could face significantly higher increases.
In a healthcare context, the same change would place a comparable burden on a charitable hospital; costs that would ultimately need to be absorbed or passed on to families.
At the same time, wider cost pressures continue to rise.
Independent charitable hospitals try to absorb some of these costs. Many reduce margins and cut back where they can.
But they cannot absorb it all. Prices have to rise if these hospitals are to remain viable.
Those fee increases force many children out of these hospitals, disrupting care pathways that families have often planned years in advance, long before these fiscal changes were introduced.
These are not short-term or easily reversible decisions. They cut across plans families have made over many years for their children’s education and wellbeing.
In healthcare, we would immediately recognise the seriousness of interrupting care pathways planned well in advance. We would not expect patients to simply absorb that disruption or start again elsewhere.
The immediate impact: disruption, uncertainty, loss of continuity
Families who were just managing are suddenly no longer able to afford the care they had planned for their child.
They are forced into difficult decisions, sometimes mid-treatment or mid-care, with no clear or suitable alternative in place. In many cases, appropriate provision is limited, and available services are already under pressure from others being displaced.
(In education, for many families, these are not new decisions; they are the unravelling of long-held plans about where and how their children would be educated).
For children, this would mean disruption to treatment, loss of continuity in care, and the stress of moving between providers at already vulnerable moments.
Now consider the system-wide impact.
Imagine if, over the course of just 12 months, more than 100 hospitals were forced to close or significantly reduce services due to this cascade of policy changes. There would be national outcry.
Yet in education, we are seeing a similarly rapid and compounding impact on schools and families, with far less attention.
Capacity in theory vs access in practice
Some families can absorb the increased costs, others are forced to move their children to other hospitals
They are assured they can be accommodated within the NHS instead.
But capacity is not always available where and when it is needed, or in the form that families require.
This is happening right now, in education.
In its written response to the Association for Families of Independent Schooling (AFIS) C.I.C. the Department for Education states that it has seen “no excessive pressure on the state-funded system” and that no local authority has suggested it is struggling to offer suitable school places. But this is a system-level assessment. It does not reflect the availability of appropriate places for individual families. And it does not reflect what we are hearing from parents.
Families are not applying to “the system” in aggregate. They are applying to specific providers, for specific courses, in specific locations, at a specific moment in their child’s education.
Evidence identified through AFIS research suggests that, particularly at post-16, students are meeting entry requirements but are not securing places at high-performing sixth forms and colleges. Demand is rising fastest at precisely the points in the system where capacity is least visible in official data.
These findings have been raised with the Department for Education. In correspondence with the Secretary of State, AFIS has highlighted pressures not yet reflected in national datasets, pointing to a growing gap between system-level assumptions and the realities experienced by families, especially at key transition points such as post-16, where provision is most constrained and demand least flexible.
There may be enough places in total, but not when and where families need it, or with the right type of provision.
In a healthcare context, even in a system under significant pressure, we would not rely solely on aggregate measures of capacity. The critical question would be whether appropriate care is available to patients, in the right place, at the right time, and for their specific needs.
System-wide and economic impact
Early evidence from Scotland, including an independent economic analysis commissioned by the Scottish Council of Independent Schools (SCIS), points to system effects following the introduction of VAT on independent school fees. Reported pupil numbers have fallen materially, particularly at key entry points, and the analysis indicates that the policy is likely to reduce, rather than increase, net public revenue over time.
Emerging evidence in England also suggests that the scale of disruption is exceeding initial government expectations. Research by AFIS indicates that around 15,000 children could face educational disruption during the 2025/26 academic year as a result of these changes, pointing to levels of displacement significantly above those anticipated in official projections prior to implementation.
While the contexts differ, this comparison highlights the risk that policy assumptions, whether in education or, by analogy, in healthcare, do not fully account for behavioural responses or system-wide consequences.
Whether in the reality of schools or the analogy of hospitals, these impacts extend beyond pupils and families.
Independent schools are significant employers and local economic contributors. Where enrolment falls or schools close, the effects are felt by staff through reduced hours and redundancies, and by the households that depend on that income. There are also wider consequences for local communities and suppliers, from catering and transport to specialist services, whose livelihoods are connected to the sector.
In healthcare, the closure or contraction of a network of providers would be recognised not only as a capacity issue, but as an economic and community issue, affecting staff, supply chains, and the resilience of local services.
These wider effects are rarely captured in headline policy assumptions, but they are an integral part of the real-world impact.
Closures, displacement, and who takes responsibility
Disruption is not hypothetical.
It is already happening.
Children are being moved mid-education, in some cases mid-academic year. Education is disrupted. Friendships are broken. Continuity of teaching and support is lost.
For families, this means making high-stakes decisions under pressure, often with limited information and no clear or suitable alternative available locally. The immediate impact is distress and uncertainty; the longer-term impact may include gaps in learning, loss of confidence, and disruption to outcomes at critical stages.
A significant number of independent schools have already closed in recent months, with sector estimates suggesting more than 80 closures over the past year.
While not all closures can be attributed to a single factor, the cumulative impact of rising costs and recent policy changes has clearly intensified the pressure on many schools.
But families report that beyond this, support is often unclear or unavailable, with local authorities frequently taking limited responsibility when places are lost, where an independent school has closed rather than a state school.
A system becoming less accessible
In some cases, families seek alternative independent schools.
But this is not always a viable option. Fee levels may be higher, and bursary or fee-assistance arrangements are not always transferable or available at the same level.
As a result, families who were previously able to access independent education through a combination of income and support are finding that this option is no longer affordable.
The effect is not simply a shift between sectors, but a narrowing of access within the independent sector itself.
Those able to absorb increased costs may remain. Those with the greatest need may still be supported in some cases.
But many middle-income families, who had previously stretched to access what they believed was the right environment for their child, are being squeezed out.
The assumptions shaping the debate
There is also a broader issue shaping this debate.
Public discussion of independent schools is often framed around a small number of high-profile institutions and a narrow perception of who attends them. This can give the impression that all independent schools are well-resourced, and that all families who use them are affluent and unaffected by cost increases.
The reality is more complex. There are over 2,500 independent schools across the UK, many of them small, specialist, or operating on tight margins. The families who access them are similarly diverse.
This also raises important questions about how assumptions about income and sector are used in public debate.
New research from AFIS highlights that there are around four times as many children from the highest-income households in the state sector as in independent schools. In fact, there are more children from these families in state schools than in the entire independent sector.
This reflects the scale of the system but challenges a common perception: socioeconomic advantage is not confined to one sector, and broad assumptions about who independent school families are do not reflect the reality.
Some families are able to pay fees comfortably. Others make significant financial sacrifices. Many rely on bursaries or fee assistance to make this choice possible.
When costs rise sharply, it is not a uniform impact.
But many of those most affected are not those typically represented in public debate.
Would we accept this reasoning in healthcare?
Why are independent schools framed as exclusive or elitist, while independent hospitals are not described in the same way?
Would we ever hear similar language used in healthcare?
Would a Health Secretary say:
“Private hospitals are businesses that can make choices about how they manage their budgets… ultimately, it’s about how attractive they are to their customers.”
Or:
“Our fiscal approach to private hospitals is designed to drive higher standards across the state system.”
These are not hypothetical arguments. They are direct adaptations of statements made by ministers in relation to independent schools.
Framed in a healthcare context, they feel deeply uncomfortable, because we instinctively recognise what is at stake.
Policy, principle, and reality
In response to questions raised by the Association for Families of Independent Schooling (AFIS), the government has been clear that it views independent schools as businesses, and that they should be treated as such.
The Department for Education has stated, “private schools, as private businesses, can decide for themselves how to manage the additional cost”.
But if other businesses, and their customers, were subject to this level of cumulative cost pressure over such a short period, it is difficult to imagine that the response from organisations such as the Confederation of British Industry or the British Chambers of Commerce would be anything other than immediate and forceful.
The Government, through the Department for Education’s response to AFIS, has also stated that it “believes in parental choice” and recognises that many parents make significant sacrifices to exercise that choice.
But meaningful choice depends on stability. Many families make educational decisions years in advance, choosing schools, planning finances, and setting expectations for their children’s future. When those plans are disrupted mid-journey, choice is not expanded; it is removed.
In practice, the effect of these changes is to reduce choice, through affordability constraints, limited availability of suitable alternatives, and capacity pressures at key transition points.
A question of consequences
When policy changes affect systems that operate alongside public provision, how carefully does government consider: – cumulative cost pressures – timing of implementation – and the real-world consequences for those relying on those services?
Because systems like this only work when all parts of them are stable.
And when that stability is disrupted, the consequences are not theoretical, they are felt in real lives.
What this means for families
This is not a debate about systems.
It is about children, families, and the stability they depend on.
Independent schools educate around 6.5% of pupils in the UK (around 600,000 children).
In a healthcare context, this would be equivalent to a group of hospitals caring for around 600,000 children.
While this represents a minority, it is a significant group of families whose needs and circumstances are no less real.
Policy decisions affecting systems of this scale should not assume that those impacted can simply be absorbed elsewhere without consequence.
Nor should these children be treated as peripheral to the system, or as a predictable outcome of policy change without adequate consideration of the impact on their education and wellbeing.
For the families affected, the impact is immediate, personal, and significant.
These are not marginal adjustments. They are decisions that reshape, and in many cases undo, plans that families have built over many years around their children’s futures.
Looking ahead
For those who believe in parental choice in education, and in the role independent schools play within it, AFIS is working to ensure that the voices of families are better heard and better represented ahead of the next general election.
As part of this, AFIS is launching a coordinated three-year programme of public affairs and communications activity through its Better Prepared campaign, focused on
ensuring that the real experiences of children and families are properly understood, evidenced, and reflected in future policy decisions.
Because decisions taken at system level should be informed by the realities faced by children and families in practice.